Acute Leukemia – Symptoms, Diagnosis, Treatment and Prognosis
Highlights of Acute Leukemia
- Acute leukemia is a blood cancer that starts in your bone marrow, where a large number of white blood cells are produced that don’t work and crowd out healthy cells.
- Symptoms of acute leukemia appear quickly and may include extreme tiredness, frequent infections, easy bruising or bleeding, bone or joint pain, pale skin, and swollen lymph nodes.
- Younger patients with acute myeloid leukemia have a better chance of long-term survival, though the risk of relapse is high.
- A bone marrow biopsy helps diagnose leukemia by collecting a small sample to check for cancerous cells, assess disease severity, and guide treatment plans.
- A stem cell transplant replaces damaged bone marrow with healthy stem cells to help restore normal blood cell production in leukemia patients, especially those with high-risk or relapsed disease.
What is Acute Leukemia?
Acute leukemia is a type of cancer that starts in your bone marrow, where your blood cells are made. In leukemia, your body quickly produces too many immature white blood cells, which don’t work properly. These abnormal cells can be either myeloid or lymphoid, leading to two main types of leukemia: acute myeloid leukemia (AML) or acute lymphoblastic leukemia (ALL). These cells can alter your immunity, making it harder for your body to fight infections, carry oxygen, or stop bleeding. [1]
Types of Acute Leukemia
Two main types of leukemia:
1. ALL
This type mainly affects lymphoid cells, a kind of white blood cell. ALL is more common in children but can also happen in adults. [2]
2. AML
This type begins in another group of blood cells, including red blood cells, platelets, and certain white blood cells. AML is more common in adults. [3]
Causes and Risk Factors of Acute Leukemia
The exact cause of acute leukemia isn’t always clear, but several factors can increase your risk:
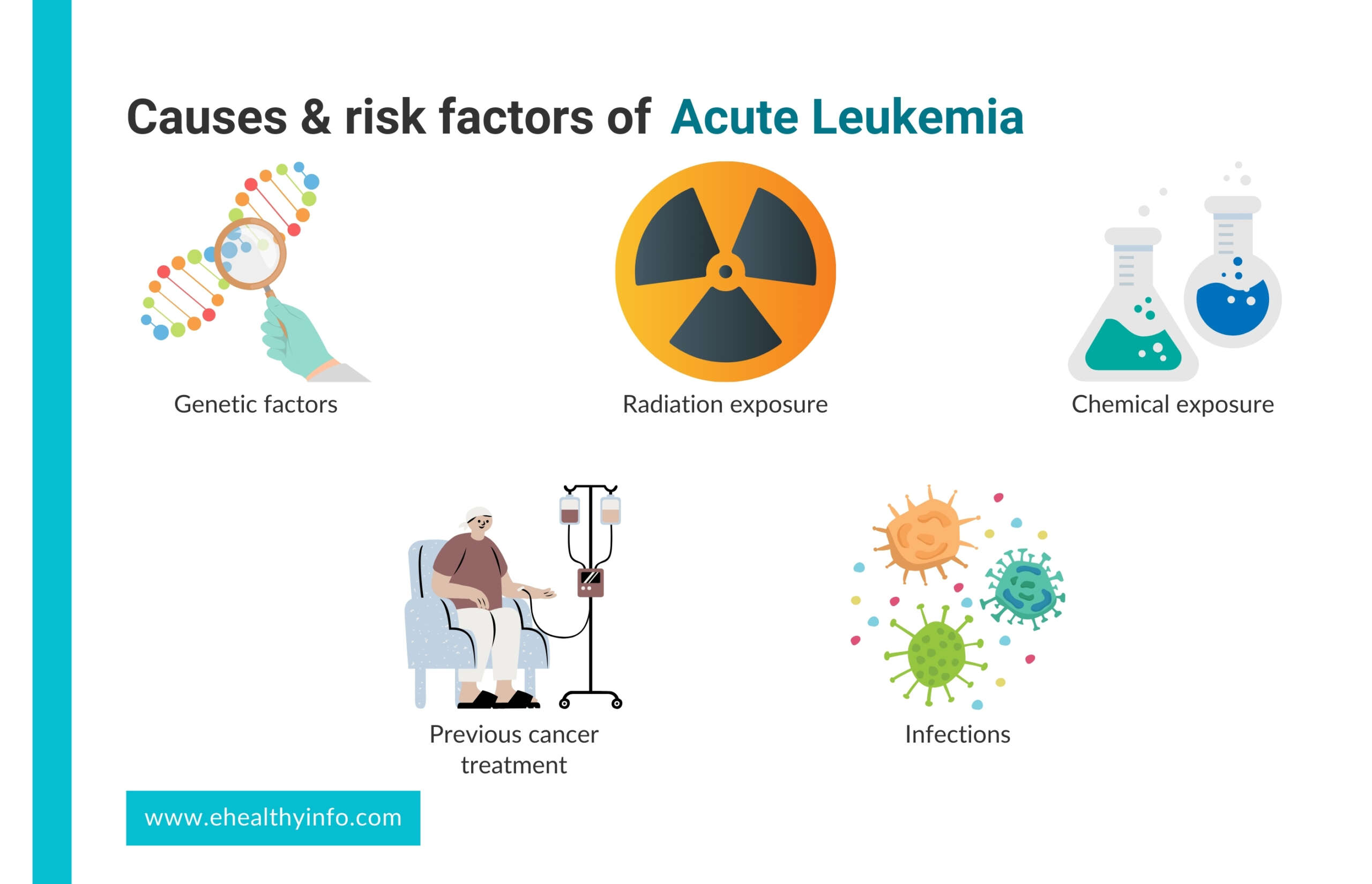
1. Genetic Factors
Genes can play a significant role in the risk of developing acute leukemia. Some inherited conditions, like Down syndrome, Li-Fraumeni syndrome, and neurofibromatosis, make it more likely to get this type of cancer. [4]
2. Radiation Exposure
Exposure to high levels of ionizing radiation, like from nuclear accidents or radiation therapy for other cancers, is strongly linked to the development of acute leukemia. [5]
3. Chemical Exposure
Long-term exposure to certain chemicals, such as benzene, which is found in industrial settings, can be a risk factor. [6]
4. Previous Cancer Treatment
Medications used in chemotherapy like melphalan, cyclophosphamide etoposide, and mitoxantrone may increase your risk of developing acute leukemia. Some of them are known to cause leukemia depending on the amount of these chemotherapy agents used and with a latency period of 5 to 7 years. [7]
5. Infections
Infections and immune system factors might contribute to the development of acute leukemia, especially in children. Some studies suggest that infections during early childhood could trigger the disease in children who are genetically more likely to develop it. [8]
Symptoms of Acute Leukemia
Acute leukemia can cause a variety of symptoms that develop quickly, often within days or weeks. Common symptoms include:
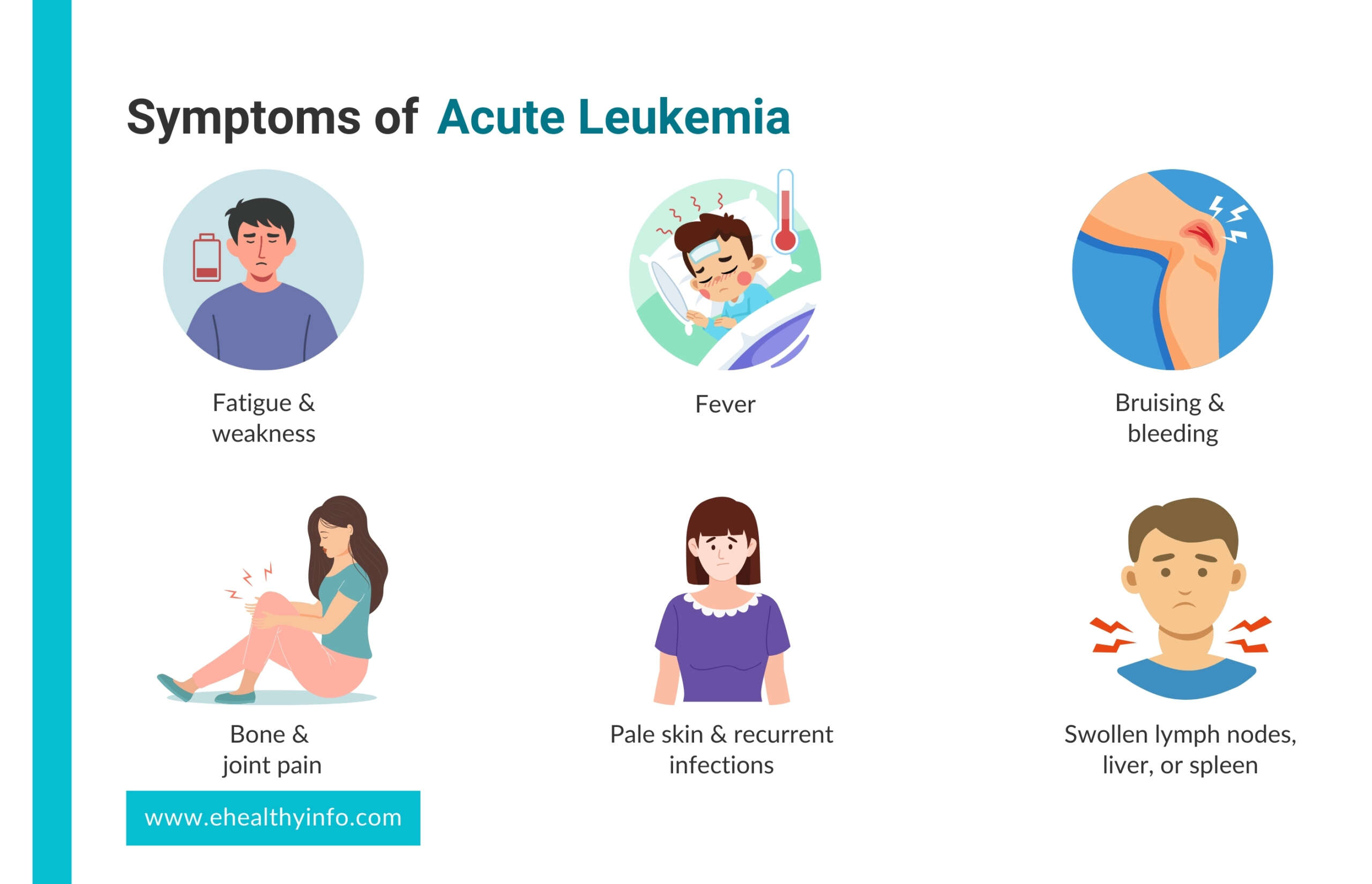
1. Fatigue and Weakness
You may feel extremely tired and weak because your bone marrow isn’t making enough red blood cells (anemia). [9]
2. Fever
You might experience persistent or recurring fevers due to leukemia or because your immune system is weakened. [10]
3. Bruising and Bleeding
It’s easier to bruise, have frequent nosebleeds or bleeding gums, or notice small red spots on your skin (petechiae) due to a low platelet count (thrombocytopenia). [10]
4. Bone and Joint Pain
As the bone marrow expands, you might feel pain in your bones or joints, especially in children. [10]
5. Pale Skin and Recurrent Infections
Your skin may look paler than usual because of anemia (a low red blood cell count), and with a low white blood cell count (leukopenia), you’re more likely to get infections.
6. Swollen Lymph Nodes, Liver, or Spleen
You could have painless lumps in your neck, armpit, or groin. You might also notice swollen lymph nodes, an enlarged liver, or an enlarged spleen. [11]
7. Weight Loss and Loss of Appetite
You could lose weight and have a reduced appetite due to the body’s increased energy needs and the disease’s impact on your digestive system.
8. Night Sweats
Though more common in chronic leukemia, night sweats can also happen in acute leukemia. [12]
Diagnosis of Acute Leukemia
If leukemia is suspected, several tests may be done depending on your symptoms and health services at your local facility.
1. Blood Tests
A complete blood count (CBC) and peripheral blood smear (PBS) are necessary tests to check for leukemia. A CBC looks at the levels of your white blood cells, red blood cells, and platelets. If you have leukemia, your white blood cell count may be too high or too low, and you might have anemia or a low platelet count. The PBS will look at your blood cells under a microscope to check for blasts (immature white blood cells) or other abnormal cells. [13]
2. Bone Marrow Aspirate and Biopsy
A bone marrow aspirate and biopsy can confirm leukemia and determine its type. In this procedure, your doctor takes a small sample of liquid bone marrow (aspirate) and a tiny piece of bone (biopsy), usually from your hip bone. These samples are examined under a microscope to check for blasts (immature white blood cells) and other abnormal cells. The test helps determine how well your bone marrow works and whether leukemia cells exist. While the procedure may cause some discomfort, it is quick and done with local anesthesia to help reduce pain. [13]
3. Flow Cytometry
Flow cytometry is a test that helps to examine your blood or bone marrow cells to identify the type of leukemia you may have. It uses a special machine that sends a stream of cells through lasers. These lasers detect specific markers on the surface of the cells, which helps doctors see whether the cells are normal or cancerous. The quick test involves drawing a small amount of blood or taking a bone marrow sample, depending on your situation. [14]
4. Lumbar Puncture
This test checks for leukemia cells in the fluid around your brain and spinal cord, especially if there’s a concern that the disease has spread to your central nervous system. [13]
5. Imaging Studies
Imaging studies help to check if leukemia has spread to different parts of your body. While leukemia mainly affects your blood and bone marrow, imaging can detect complications like infections, enlarged organs, or leukemia spreading to the brain, chest, or bones. A chest X-ray is often used to check for swollen lymph nodes or lung infections. A Computed Tomography (CT) scan or Magnetic Resonance Imaging (MRI) provides detailed images of your organs, helping to see if leukemia has affected your liver, spleen, or brain. Sometimes, a Positron Emission Tomography (PET) scan can detect active cancer cells. While imaging isn’t used to diagnose leukemia, it helps doctors assess your overall health and plan the best treatment. [15]
6. Genetic Tests or Karyotyping
Genetic tests help doctors understand changes in leukemia cells that affect diagnosis, treatment, and prognosis. Karyotyping is a type of genetic test that checks for missing or extra chromosome parts. At the same time, Fluorescence In Situ Hybridization (FISH) highlights specific genetic changes that may not be visible in karyotyping. Next-Generation Sequencing (NGS) goes even deeper, detecting small gene mutations that influence how leukemia grows and which treatments may work best. [16]
Treatment of Acute Leukemia
Phase of treatment: The treatment of acute leukemia, including both AML and ALL, usually happens in several stages:
Induction Therapy
In this first phase, the goal is to reduce the number of leukemia cells in your body to an undetectable level and help your body start producing normal blood cells again. [17]
Consolidation Therapy
After you reach remission (when the cancer isn’t detectable), consolidation therapy works to eliminate any remaining leukemia cells to prevent the cancer from coming back. In AML, this might involve high-dose chemotherapy or a stem cell transplant if you’re at high risk. In ALL, you’ll likely go through more chemotherapy, and you might also receive treatment to protect your brain and spinal cord from leukemia. [18]
Maintenance Therapy
Maintenance therapy is often used in ALL to keep the leukemia in remission. This phase involves taking lower doses of chemotherapy over a long period, usually 2-3 years. [18]
CNS-Directed Therapy
If you have ALL, it’s important to protect your brain and spinal cord because leukemia can spread there. During your treatment, you might receive chemotherapy directly into the fluid around your spinal cord or undergo radiation therapy to the brain to prevent this. [19] Treatment options: Treatment often involves a combination of therapies
1. Chemotherapy
Chemotherapy is the primary treatment for leukemia, using powerful drugs to destroy cancer cells in your blood and bone marrow. These drugs can be given as pills, injections, or through an IV. The treatment is usually given in cycles to allow your body time to recover. While chemotherapy effectively kills leukemia cells, it can also affect healthy cells, leading to side effects like fatigue, nausea, hair loss, and a weakened immune system. In some cases, doctors combine different chemotherapy drugs or use them alongside other treatments like targeted therapy or a stem cell transplant to improve results. Chemotherapy that might be used is daunorubicin. Cytarabine, and vincristine. [20]
2. Targeted Therapy
Targeted therapy is a treatment for leukemia that uses special drugs to attack cancer cells while causing less harm to normal cells. Unlike chemotherapy, which affects all rapidly growing cells, targeted therapy focuses on specific proteins or genes that help leukemia cells grow. These drugs can block signals that allow cancer to spread, cut off its blood supply, or help the immune system destroy cancer cells. Common types include FLT3 inhibitors like midostaurin and gilteritinib, IDH1/2 inhibitors like ivosidenib and enasidenib, and BCL-2 inhibitors like venetoclax. Targeted therapy is often used alone or combined with chemotherapy to improve treatment outcomes. [21]
3. Radiation Therapy
Radiation therapy uses high-energy rays to kill or stop leukemia cells from growing. While leukemia mainly affects the blood and bone marrow, radiation may be used in specific cases, such as when leukemia has spread to the brain, spinal cord, or lymph nodes. It can also be part of treatment before a stem cell transplant to help destroy remaining cancer cells. The procedure is painless and typically given in short sessions over several days. Depending on the area treated, common side effects include fatigue, skin irritation, and nausea. Radiation is often combined with other treatments like chemotherapy for better results. [22]
4. Stem Cell Transplant
Stem cell transplant replaces damaged bone marrow with healthy stem cells. It is usually done after high-dose chemotherapy or radiation, which destroys both cancerous and healthy cells in the bone marrow. The new stem cells, either from a donor (allogeneic transplant) or the patient’s own body(autologous transplant), help rebuild healthy blood cells. This procedure can improve the chances of remission, especially in aggressive or relapsed leukemia. However, it carries risks like infections, graft-versus-host disease (if donor cells attack the body), and a lengthy recovery period. Stem cell transplants are often used when other treatments are not enough to cure leukemia. [23]
Complications of Acute Leukemia
Acute leukemia can lead to various complications, both from the disease itself and its treatment.
1. Blood-Related Complications
- Tumor Lysis Syndrome: This happens when cancer cells break down quickly, releasing substances into the blood that can cause high levels of uric acid, potassium, and phosphate and low calcium levels. [24]
- Hyperleukocytosis and Leukostasis: High white blood cell counts can clog blood vessels, leading to breathing problems and neurological symptoms. [25]
- Thrombohemorrhagic Syndromes: Particularly in acute promyelocytic leukemia (APL), you may experience severe bleeding or clotting due to issues like disseminated intravascular coagulation (DIC). [26]
2. Infectious Complications
Infectious complications are common due to low white blood cell counts and weakened immunity. Neutropenic fever can occur when your body has too few infection-fighting cells, putting you at high risk for serious infections that require immediate antibiotic treatment. Opportunistic infections, including fungal, viral, and bacterial infections, can also develop due to prolonged immunosuppression from leukemia or its treatments. [27]
3. Neurologic Complications
Leukemia can affect your nervous system, leading to serious complications. Leukemic meningitis occurs when leukemia cells spread to the brain and spinal cord, causing symptoms like headaches, nausea, vision changes, and confusion, similar to meningitis. Chemotherapy-induced neurotoxicity happens when certain chemotherapy drugs, like cytarabine, affect the brain and nervous system. This can lead to cerebellar toxicity, which causes problems with coordination and balance, or encephalopathy, which results in confusion and altered mental function. [28]
4. Heart-Related Complications
Some chemotherapy drugs, especially anthracyclines like doxorubicin, can weaken the heart muscle over time, leading to cardiomyopathy or heart failure. Radiation therapy to the chest may also damage the heart and blood vessels, increasing the risk of coronary artery disease or irregular heart rhythms (arrhythmias). [29]
5. Digestive System Complications
Chemotherapy and radiation can damage the lining of your digestive tract, causing nausea, vomiting, diarrhea, or constipation. Some treatments may also lead to mucositis, which causes painful sores in the mouth and throat, making it difficult to eat and swallow. Some chemotherapy drugs can inflame the liver and pancreas, especially in children. Additionally, chemotherapy can affect your liver, leading to liver toxicity or abnormal liver function. Weakened immunity increases the risk of gut infections, which can cause severe diarrhea, dehydration, and even sepsis. [30]
Prognosis of Acute Leukemia
The outlook for acute leukemia depends on factors like your age, genetic makeup, and response to treatment.
- AML: If you’re under 60, chemotherapy can lead to remission in about 70-80% of cases, but there’s still a high chance of relapse. Long-term survival improves with additional treatments like high-dose chemotherapy or a stem cell transplant, especially for high-risk patients. For those over 60, remission rates drop to about 50%, and relapse is very common within three years. Unfortunately, only 5-8% of older adults survive beyond five years due to other health conditions and genetic factors. [19]
- ALL: The prognosis is much better for children, with about 90% surviving at least five years. Adolescents and young adults also have a good outlook, with around 60% surviving five years or more. However, for adults, the survival rate drops to 20-40%, and for those over 40, it’s even lower, with only about 20% surviving beyond five years. Early diagnosis and aggressive treatment play a key role in improving outcomes. [19]
Questions To Ask Your Doctor
- How will having acute leukemia change my daily life and activities?
- What are the chances that the leukemia will come back after treatment?
- How often will I need to have check-ups and monitoring after my treatment for acute leukemia?
- Are there any specific foods I should eat or avoid while I have acute leukemia?
- How can I stay physically healthy and fit during and after my treatment for acute leukemia?
Conflict of Interest
PK is a research assistant at eHealthyInfo and receives compensation for her work.
References
- Ladikou EE, Ashworth I, Seviar D, Chevassut T. Acute leukaemia: no reason to panic. Clinical Medicine. 2022 May;22(3):221–4. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9135077/
- Gbenjo JTC, McCrary GLM, Wilson SE. Leukemia: What Primary Care Physicians Need to Know. American Family Physician [Internet]. 2023 Apr 1;107(4):397–405. Available from: https://pubmed.ncbi.nlm.nih.gov/37054416/
- Davis AS, Viera AJ, Mead MD. Leukemia: an overview for primary care. American Family Physician [Internet]. 2014 May 1;89(9):731–8. Available from: https://pubmed.ncbi.nlm.nih.gov/24784336/
- Brown PA, Shah B, Advani A, Aoun P, Boyer MW, Burke PW, et al. Acute Lymphoblastic Leukemia, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network. 2021 Sep;19(9):1079–109. Available from: https://pubmed.ncbi.nlm.nih.gov/34551384/
- Kosik P, Skorvaga M, Igor Belyaev. Preleukemic Fusion Genes Induced via Ionizing Radiation. International Journal of Molecular Sciences [Internet]. 2023 Apr 1 [cited 2024 Feb 18];24(7):6580–0. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10095576/
- Vivarelli S, Sevim C, Giambò F, Fenga C. Integrated Computational Analysis Reveals Early Genetic and Epigenetic AML Susceptibility Biomarkers in Benzene-Exposed Workers. International journal of molecular sciences [Internet]. 2025;26(3):1138. Available from: https://pubmed.ncbi.nlm.nih.gov/39940906/
- Lomov NA, Viushkov VS, Rubtsov MA. Mechanisms of Secondary Leukemia Development Caused by Treatment with DNA Topoisomerase Inhibitors. Biochemistry Biokhimiia [Internet]. 2023 Jul;88(7):892–911. Available from: https://pubmed.ncbi.nlm.nih.gov/37751862/
- Tebbi CK. Etiology of Acute Leukemia: A Review. Cancers [Internet]. 2021 Jan 1;13(9):2256. Available from: https://www.mdpi.com/2072-6694/13/9/2256
- Clarke RT, Van den Bruel A, Bankhead C, Mitchell CD, Phillips B, Thompson MJ. Clinical presentation of childhood leukaemia: a systematic review and meta-analysis. Archives of Disease in Childhood. 2016 Sep 19;101(10):894–901. Available from: https://pubmed.ncbi.nlm.nih.gov/27647842/
- Shephard EA, Neal RD, Rose PW, Walter FM, Hamilton W. Symptoms of adult chronic and acute leukaemia before diagnosis: large primary care case-control studies using electronic records. British Journal of General Practice. 2016 Feb 25;66(644):e182–8. Available from: https://pubmed.ncbi.nlm.nih.gov/26917658/
- Biswas S, Chakrabarti S, Chakraborty J, Paul PC, Konar A, Das S. Childhood acute leukemia in West Bengal, India with an emphasis on uncommon clinical features. Asian Pacific journal of cancer prevention : APJCP [Internet]. 2009;10(5):903–6. Available from: https://pubmed.ncbi.nlm.nih.gov/20104987/
- Howell DA, Warburton F, Ramirez AJ, Roman E, Smith AG, Forbes LJL. Risk factors and time to symptomatic presentation in leukaemia, lymphoma and myeloma. British Journal of Cancer. 2015 Sep;113(7):1114–20. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4651121/
- de Haas V, Ismaila N, Advani A, Arber DA, Dabney RS, Patel-Donnelly D, et al. Initial Diagnostic Work-Up of Acute Leukemia: ASCO Clinical Practice Guideline Endorsement of the College of American Pathologists and American Society of Hematology Guideline. Journal of Clinical Oncology [Internet]. 2019 Jan 20;37(3):239–53. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6338392/
- Ally F, Chen X. Acute Myeloid Leukemia: Diagnosis and Evaluation by Flow Cytometry. Cancers. 2024 Nov 17;16(22):3855–5. Available from: https://pubmed.ncbi.nlm.nih.gov/39594810/
- Pollyea DA, Altman JK, Assi R, Bixby D, Fathi AT, Foran JM, et al. Acute Myeloid Leukemia, Version 3.2023, NCCN Clinical Practice Guidelines in Oncology. 2023 May 1;21(5):503–13. Available from: https://pubmed.ncbi.nlm.nih.gov/37156478/
- Harris MH, Czuchlewski DR, Arber DA, Czader M. Genetic Testing in the Diagnosis and Biology of Acute Leukemia. American Journal of Clinical Pathology. 2019 Jul 2;152(3):322–46.Available from: https://pubmed.ncbi.nlm.nih.gov/31367767/
- Lechner. Treatment of acute leukemia. Annals of oncology : official journal of the European Society for Medical Oncology [Internet]. 2024 [cited 2024 Sep 4];10 Suppl 6. Available from: https://pubmed.ncbi.nlm.nih.gov/10676552/
- Pratz KW, Cherry M, Altman JK, Cooper BW, Podoltsev NA, Jose Carlos Cruz, et al. Gilteritinib in Combination With Induction and Consolidation Chemotherapy and as Maintenance Therapy: A Phase IB Study in Patients With Newly Diagnosed AML. Journal of Clinical Oncology. 2023 Sep 10;41(26):4236–46. Available from: https://pubmed.ncbi.nlm.nih.gov/37379495/
- Burnett A, Wetzler M, Löwenberg B. Therapeutic Advances in Acute Myeloid Leukemia. Journal of Clinical Oncology. 2011 Feb 10;29(5):487–94. Available from: https://pubmed.ncbi.nlm.nih.gov/21220605/
- Jaramillo S, Schlenk RF. Update on current treatments for adult acute myeloid leukemia: to treat acute myeloid leukemia intensively or non-intensively? That is the question. Haematologica. 2023 Feb 1;108(2):342–52. Available from: https://pubmed.ncbi.nlm.nih.gov/36722404/
- Kantarjian HM, Kadia TM, DiNardo CD, Welch MA, Ravandi F. Acute myeloid leukemia: Treatment and research outlook for 2021 and the MD Anderson approach. Cancer. 2021 Mar 18;127(8):1186–207. Available from: https://pubmed.ncbi.nlm.nih.gov/33734442/
- Bodet-Milin C, Kraeber-Bodéré F, Eugène T, Guérard F, Gaschet J, Bailly C, et al. Radioimmunotherapy for Treatment of Acute Leukemia. Seminars in Nuclear Medicine [Internet]. 2016 Mar 1 [cited 2021 Dec 16];46(2):135–46. Available from: https://pubmed.ncbi.nlm.nih.gov/26897718/
- Stubbins RJ, Francis A, Kuchenbauer F, Sanford D. Management of Acute Myeloid Leukemia: A Review for General Practitioners in Oncology. Current Oncology [Internet]. 2022 Aug 30;29(9):6245–59. Available from: https://pubmed.ncbi.nlm.nih.gov/36135060/
- Xue Y, Chen J, Gao S, Zhai X, Wang N, Gao J, et al. Clinical characteristics of tumor lysis syndrome in childhood acute lymphoblastic leukemia. Scientific Reports. 2021 May 6;11(1). Available from: https://pubmed.ncbi.nlm.nih.gov/33958615/
- Giammarco S, Chiusolo P, Piccirillo N, Di Giovanni A, Metafuni E, Laurenti L, et al. Hyperleukocytosis and leukostasis: management of a medical emergency. Expert Review of Hematology. 2016 Dec 26;10(2):147–54. Available from: https://pubmed.ncbi.nlm.nih.gov/27967252/
- Paterno G, Palmieri R, Cristiano Tesei, Nunzi A, Ranucci G, Mallegni F, et al. The ISTH DIC-score predicts early mortality in patients with non-promyelocitic acute myeloid leukemia. Thrombosis Research. 2024 Feb 16;236:30–6. Available from: https://pubmed.ncbi.nlm.nih.gov/38387301/
- Zając-Spychała O, Skalska-Sadowska J, Wachowiak J, Szmydki-Baran A, Hutnik Ł, Matysiak M, et al. Infections in children with acute myeloid leukemia: increased mortality in relapsed/refractory patients. Leukemia & Lymphoma. 2019 May 28;60(12):3028–35. Available from: https://pubmed.ncbi.nlm.nih.gov/31132917/
- Baloda R, Sharma S, Anand R, Mandal P, Parakh N, Katti B, et al. Neurologic Complications in Patients With Lymphoreticular Malignancy: A Descriptive Cohort Study. Journal of Pediatric Hematology/Oncology. 2023 Jul 24;45(7):e885–91. Available from: https://pubmed.ncbi.nlm.nih.gov/37526372/
- Assuncao BMBL, Handschumacher MD, Brunner AM, Yucel E, Bartko PE, Cheng KH, et al. Acute Leukemia is Associated with Cardiac Alterations before Chemotherapy. Journal of the American Society of Echocardiography. 2017 Nov;30(11):1111–8. Available from: https://pubmed.ncbi.nlm.nih.gov/28927558/
- Rocka A, Woźniak M, Lejman M, Zawitkowska J. Severe complications in the induction phase of therapy in a pediatric patient with T-cell acute lymphoblastic leukemia: A case report. Medicine. 2023 Sep 8;102(36):e34965. Available from: https://pubmed.ncbi.nlm.nih.gov/37682188/