Reactive Arthritis – Symptoms, Diagnosis, Treatment, and Prevention

Highlights of Reactive Arthritis
- Reactive Arthritis is joint pain that occurs when the immune system reacts to an infection elsewhere in the body, such as the intestines or urinary tract. It is commonly triggered by infections from bacteria like Salmonella, Chlamydia, and Campylobacter.
- HLA-B 27 is the most common gene associated with reactive arthritis; however, not all people with this gene will have reactive arthritis.
- Reactive arthritis’s symptoms are not limited to the joint and can cause high inflammation, urinary problems, and skin rashes.
- An anti-inflammatory diet rich in omega-3 fatty acids (fish), fruits, vegetables, whole grains and low in processed foods can help manage symptoms and overall health.
- Practicing good hygiene, protection during sexual activity, and treating infections with appropriate antibiotics can help prevent reactive arthritis.
What is Reactive Arthritis?
Reactive Arthritis is an autoimmune condition that occurs when the body reacts to an infection in another part of the body, like gastroenteritis or a sexually transmitted infection. The immune system mistakenly attacks joints, making them swollen and painful. It usually affects large joints, like knees, and starts about 2-4 weeks after the infection.[1,2]
Causes of Reactive Arthritis
Common Causes and Triggers of Reactive Arthritis:
- Infections: Salmonella, Shigella, Chlamydia, and Campylobacter are common bacteria that can trigger ReA. These bacteria leave behind parts of themselves in the joints, which can provoke the immune system.[3]Additionally, Human immunodeficiency virus (HIV) infection can increase the risk of reactive arthritis.
- Genetics: Reactive arthritis is often linked to genetics, with the HLA-B27 gene being a major risk factor. Around 50-80% of people with reactive arthritis carry this gene, but not everyone with HLA-B27 develops the condition. A family history of HLA-B27-associated diseases also raises the risk, highlighting the genetic influence on reactive arthritis. [4]
Symptoms of Reactive Arthritis
Reactive arthritis usually shows up with a mix of joint-related and other symptoms:
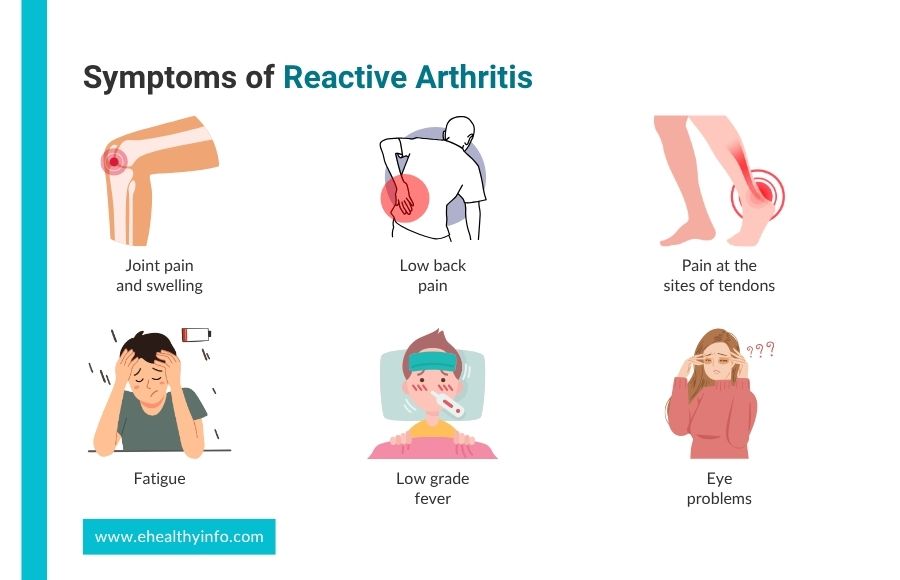
1. Joint Pain and Swelling
Reactive arthritis often causes inflammation in a small number of joints, typically affecting the lower limbs like the knees, ankles, and feet the most. This is the main sign of reactive arthritis. Fingers or toes may swell up, giving them a “sausage digit” appearance. [5]
2. Low Back Pain
Lower back pain due to inflammation in the sacroiliac joints is also one of the symptoms of Reactive arthritis. This type of pain starts gradually, often with stiffness in the lower back in the morning that gets better with movement. Unlike regular back pain, it improves with activity and can disturb sleep, especially later in the night. [6]
3. Pain at The Sites of Tendons
People may experience pain and tenderness at the sites where tendons connect to bones. Achilles tendon and plantar fascia are the most common areas of pain affecting your daily activities and causing functional limitations. [7]
4. Non-Joint-Related Symptoms
Reactive arthritis can cause various non-joint-related symptoms affecting other body parts. Fatigue is a common issue, often accompanied by low-grade fever. This condition can also lead to eye problems such as dryness, inflammation, and sensitivity to light. [8] The lungs may be affected, causing interstitial lung disease or pleuritis, leading to shortness of breath or chest pain. It may cause skin nodules, particularly near the elbows or fingers.
Diagnosis of Reactive Arthritis
There is no single test for diagnosing reactive arthritis. Common tests include:
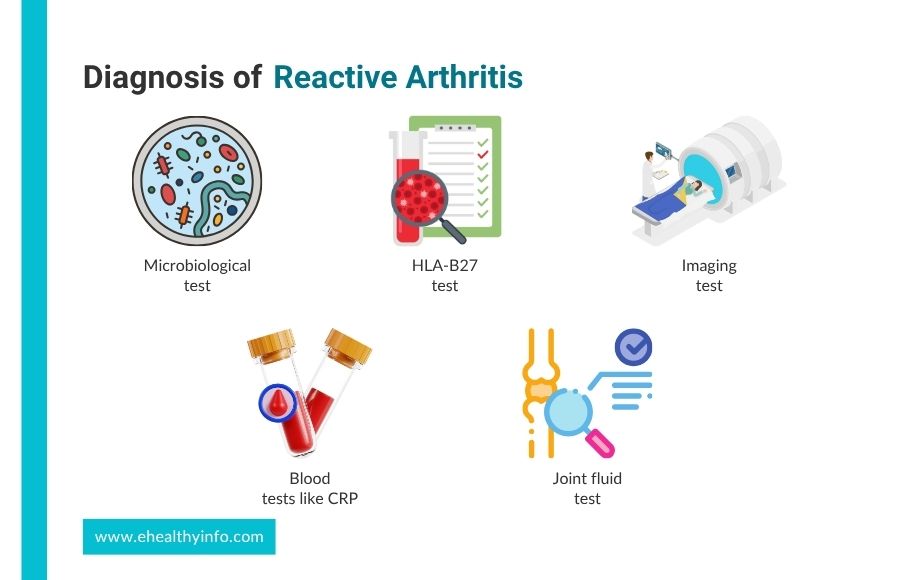
Laboratory Tests
- Microbiological Test: Stool cultures find enteric pathogens like Salmonella, Shigella, Campylobacter, or Yersinia. Urogenital swabs are tested using nucleic acid amplification tests (NAAT) to detect Chlamydia trachomatis.
- Blood Test: Blood tests help identify signs of inflammation, genetic predispositions, and recent infections. Common tests include measuring inflammatory markers like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), often elevated due to the body’s inflammatory response. Additionally, blood tests can detect antibodies indicating recent bacterial infections by pathogens such as Chlamydia trachomatis, Salmonella, Shigella, Yersinia, or Campylobacter. A complete blood count (CBC) may assess overall health and rule out other conditions.
- HLA-B27 Test: It detects the presence of the HLA-B27 gene, associated with an increased risk of developing reactive arthritis and other autoimmune conditions. [4]
- Imaging: X-rays or MRIs may assess joint damage or inflammation, though these changes are often subtle or absent in early reactive arthritis.
- Joint Fluid Test: This test involves taking fluid from an affected joint to study its characteristics in a lab. It helps rule out other types of arthritis, like those caused by infections or gout. The tests look at inflammation levels, check for bacteria, and examine crystals that can indicate different kinds of arthritis. It rules out septic arthritis and crystalline arthritis. [9]
Treatment of Reactive Arthritis
Treatment of reactive arthritis includes:
1. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
These are usually the first choices to manage the inflammation and pain. They help reduce swelling and inflammation.[10]
2. Antibiotics
If reactive arthritis is caused by an STI, antibiotics like doxycycline, erythromycin, and azithromycin are used. Treatment of sexual partners at the same time is important to prevent reinfection.[11]
3. Corticosteroids
If NSAIDs don’t help, corticosteroid injections into the joints can reduce inflammation. Your doctor might prescribe corticosteroids to reduce the symptoms for more severe cases.
4. Disease-Modifying Antirheumatic Drugs (DMARDs)
If you have had reactive arthritis for a long time, especially if it has been present for more than six months, disease-modifying drugs like sulfasalazine may be used. In severe cases, other medications, such as methotrexate and azathioprine, may be used.
5. Biologic Agents
Sometimes reactive arthritis gets so severe that they need stronger agents to control the symptoms. Biologic agents like etanercept and infliximab are commonly used effective groups of medications.[12]
6. Physiotherapy
Physiotherapy helps prevent muscles from weakening and keeps joints flexible. These therapies include exercises to help maintain range of motion, strength, and muscles and improve overall fitness. One common type of exercise, low blood-floor restricted resistance training, has been shown to be helpful in reactive arthritis.
7. Lifestyle Modification
Maintaining a healthy weight is important to avoid extra stress on the joints, and an anti-inflammatory diet rich in fruits, vegetables, whole grains, and omega-3 fatty acids can help reduce inflammation. Adequate rest is essential for recovery, but avoiding prolonged inactivity is key to preventing stiffness. Managing stress through mindfulness or yoga, quitting smoking, and reducing alcohol intake can also enhance overall well-being and treatment effectiveness. [13]
8. Footwear
Shoes designed for arthritis, whether custom-made or off-the-shelf, can significantly reduce foot pain and improve mobility by providing better support. They help distribute pressure evenly and lessen strain on your joints. Using special inserts in these supportive shoes can reduce pain and discomfort, making it easier to move feet and toes. [14]
How to Prevent Reactive Arthritis?
Preventing reactive arthritis primarily involves managing the risk of infections that can trigger the condition. Good hygiene, such as regular handwashing and safe food handling, helps prevent gastrointestinal infections from bacteria like Salmonella and Shigella. Protecting yourself during sexual activity can reduce the risk of genitourinary infections, such as Chlamydia, which are linked to reactive arthritis. Prompt treatment of infections with appropriate antibiotics or medications is crucial to minimize the risk of developing reactive arthritis.
Pregnancy and Reactive Arthritis
During pregnancy, reactive arthritis should be carefully managed to minimize risks such as preterm delivery and low birth weight. Certain medications, like methotrexate and leflunomide, should be stopped before conception due to their potential harm to the baby. Safer alternatives, such as corticosteroids and other medications, are preferred. Biologic agents, like certolizumab, may be cautiously used, especially early in pregnancy. Regular monitoring is important to address maternal complications like hypertension and blood clotting, as well as fetal growth problems. [15–17]
Questions To Ask Your Doctor
- What are the potential complications if reactive arthritis is left untreated?
- How would I know if my condition is worsening?
- When should I seek immediate medical attention?
- How can I manage flare-ups and prevent them from worsening?
- What is the long-term outlook for someone with reactive arthritis?
References
- Hannu T, Inman R, Granfors K, Leirisalo-Repo M. Reactive arthritis or post-infectious arthritis? Best Pract Res Clin Rheumatol 2006;20:419–33. https://doi.org/10.1016/J.BERH.2006.02.003.
- Flores D, Marquez J, Garza M, Espinoza LR. Reactive arthritis: newer developments. Rheum Dis Clin North Am 2003;29:37–59. https://doi.org/10.1016/S0889-857X(02)00081-9.
- Keat A. Reactive arthritis. Adv Exp Med Biol 1999;455:201–6. https://doi.org/10.1007/978-1-4615-4857-7_29.
- Bentaleb I, Kawther &, Abdelghani B, Rostom S, Amine B, Laatar A, et al. Reactive Arthritis: Update n.d. https://doi.org/10.1542/PEDS.2014-0623
- Jubber A, Moorthy A. Reactive arthritis: a clinical review. J R Coll Physicians Edinb 2021;51:288–97. https://doi.org/10.4997/JRCPE.2021.319.
- Selmi C, Gershwin ME. Diagnosis and classification of reactive arthritis. Autoimmun Rev 2014;13:546–9. https://doi.org/10.1016/J.AUTREV.2014.01.005.
- D’Agostino MA, Olivieri I. Enthesitis. Best Pract Res Clin Rheumatol 2006;20:473–86. https://doi.org/10.1016/J.BERH.2006.03.007.
- Ngaruiya CM, Martin IBK. A case of reactive arthritis: a great masquerader. Am J Emerg Med 2013;31:266.e5-266.e7. https://doi.org/10.1016/J.AJEM.2012.04.019.
- Courtney P, Doherty M. Joint aspiration and injection and synovial fluid analysis. Best Pract Res Clin Rheumatol 2009;23:161–92. https://doi.org/10.1016/J.BERH.2009.01.003.
- Rudwaleit M, Braun J, Sieper J. Treatment of reactive arthritis: a practical guide. BioDrugs 2000;13:21–8. https://doi.org/10.2165/00063030-200013010-00003.
- Barber CE, Kim J, Inman RD, Esdaile JM, James MT. Antibiotics for treatment of reactive arthritis: a systematic review and metaanalysis. J Rheumatol 2013;40:916–28. https://doi.org/10.3899/JRHEUM.121192.
- Colmegna I, Espinoza LR. Recent advances in reactive arthritis. Curr Rheumatol Rep 2005;7:201–7. https://doi.org/10.1007/S11926-996-0040-4.
- Nikiphorou E, Philippou E. Nutrition and its role in prevention and management of rheumatoid arthritis. Autoimmun Rev 2023;22. https://doi.org/10.1016/J.AUTREV.2023.103333.
- Riskowski J, Dufour AB, Hannan MT. Arthritis, foot pain and shoe wear: current musculoskeletal research on feet. Curr Opin Rheumatol 2011;23:148–55. https://doi.org/10.1097/BOR.0B013E3283422CF5.
- Skorpen CG, Hoeltzenbein M, Tincani A, Fischer-Betz R, Elefant E, Chambers C, et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann Rheum Dis 2016;75:795–810. https://doi.org/10.1136/ANNRHEUMDIS-2015-208840.
- Sammaritano LR, Bermas BL, Chakravarty EE, Chambers C, Clowse MEB, Lockshin MD, et al. 2020 American College of Rheumatology Guideline for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases. Arthritis Care Res (Hoboken) 2020;72:461–88. https://doi.org/10.1002/ACR.24130.
- Nalli C, Galli J, Lini D, Merlini A, Piantoni S, Lazzaroni MG, et al. The Influence of Treatment of Inflammatory Arthritis During Pregnancy on the Long-Term Children’s Outcome. Front Pharmacol 2021;12. https://doi.org/10.3389/FPHAR.2021.626258.